


Authors:
Gábor Varga (Introduction)
Dr. Tamás Ugrai
Anita Varga
Table of contents
Summary
Introduction / Gábor Varga
Description of the proinsulin C peptide spray
Description of the study
The number, sex, age and comorbidity of the investigated participants
The group of patients with frequent symptoms
Group of patients with moderately frequent symptoms
Group of patients with rare symptoms
Investigation of comorbidity and returning to work
Most frequently used antibiotic and antiviral drugs, supplementary treatments
Literature related to the present investigation
Summary
In December 2019 a new type of coronavirus the SARS-CoV-2 appeared in China, which caused a disease named Covid–19. Since the outbreak of the Covid–19 pandemic, international studies proved consistently that the pathogenic effect is achieved primarily through attacking and damaging the immune system. The virus gets into the cells predominantly bound to the ACE2 enzyme receptor located in the epithelial cells covering the alveoli of the lung. This receptor appears not only in the cells of the lung, but also in the epithelial cells of the myocardium, the kidney, the esophagus, the stomach and the intestines, the cells lining the blood vessels as well as on the surface of certain leukocytes. As a consequence general inflammations evolve and these cause the so called „cytokine storm”, the increased production of inflammatory proteins.
The disturbance of the cytokine network plays an important role in the development of the clinical symptoms and the prognosis of the disease.
After becoming infected a number of patients remain symptom free or only mild symptoms appear. Meanwhile in a higher percentage of the infected persons, mainly in the elderly and patients suffering from comorbidities severe condition is developed frequently, which may have fatal outcome due to respiratory failure on one hand and septic shock on the other hand as a consequence of the bacterial superinfection.
According to the clinical significance the temporal course of Covid–19 can be divided into 3 phases:
I. phase (early phase of the infection):
- respiratory
- gastro-enteric symptoms
- high fever
II. phase (phase of lungs complications)
- pneumonia is developed
III. phase
- development of systemic inflammation, cytokine storm with diverse clinical symptoms, appearance of MAS (macrophage activation syndrome) and HLH (hemophagocytic lymphohistiocytosis.
The adult HLH virus infections can raise the number of autoimmune, malignant, hematopoietic, neurological, hormonal and psychic diseases or worsen the state of the existing ones.
Due to the abnormal immune functioning the lungs, heart, kidney, brain, digestive system get sick, also causing endothel damage to the blood vessels of the target organs, which cause a number of irreversible symptoms specific to the affected organ. This process destroys the quality of life, makes life expectancy shorter, regardless of age, even in young ages.
Increase of blood pressure, decrease of pulse and HRV values by approximately 30% can predict the development of the disease in several cases, or it can refer to the presence of the virus.
HRV value: the responsiveness of the heart, means the whole person’s emotional, hormonal, neural balance and the reactivity to situations of life. The higher value of heart rate variability (HRV) is a complex measure of health. It describes how can the heart constantly change the period between one to another heartbeat, reacting to the varying loads of the internal and external environment. The adaptability of the heart is based on the optimal interplay of the sympathetic and parasympathetic nervous system. Appropriate heart rate variability can be achieved in the body if there is balance between the two systems. If the sympathetic system is predominated, the HRV value will decrease. This than increases the risk of developing cardiovascular diseases.
The most appropriate phrase for the prime attack to the immune system is the cytokine storm, and these mean the worst consequences, causing acute mortality.
Our testing concerning the effectiveness of C-peptide proved its favourable effect on the immune system and its functioning in our studies. Therefore in our present investigation we tested the use of intranasal C-peptide in 30 cases being positive in Covid-19 testing or showing the symptoms of Covid-19.
In our present investigation we were focusing on the answers to the following questions:
- What was the percentage of the different symptoms in the patients with a positive Covid-19 test?
- What was the percentage of comorbidities?
- What was the distribution of sexes among the 30 participants?
- What kind of treatments were needed during the process of recovery?
- Apart from general therapy what kind of supplementary treatment was applied?
- Did they need hospitalization?
- What was the length of recovery while applying the spray?
Since we are aware of the possible complications, we find it necessary plan to follow up the patients in 2 and in 6 months time, since it is known from our previous studies that C-peptide is highly effective in inhibiting the later consequences due to the abnormal functioning of the immune system, which has an estimated risk of 60 percent according to the literature. The question is whether the percentage of the risk to develop complications will change favorably due to the C-peptide treatment. Unfortunately the known consequences lead to very severe harm to health, irreversible disability or even fatal outcome.
The verbal feed-back of the investigated patients expressed a concordant opinion , that the above described symptoms rapidly relieved after introducing the c-peptide treatment, therefore their well-being significantly improved, also their hope for recovery. None of those who were treated with C-peptide were observed to have the most severe complications.
Introduction / Gábor Varga
The importance of central proinsulin C peptide in the treatment of COVID-19
The increase of the inflammatory markers CRP and Il-6 predict the unfavorable course of the covid-19 infection. [i] [ii] The decrease of HRV by more than 40% precedes a 50% increase in CRP during the next 72 hours according to a small study. [iii] The sudden decrease of HRV may signal the weakening or collapse of the cholinergic anti-inflammatory pathway. It is supposed that by strengthening this pathway the cytokine storm could be prevented or at least mitigated. [iv] [v][vi] In an animal study it was shown that increased vagus nerve activity, measured by (RMSSD), the parasympathetic part of the HRV, the brain inflammatory processes, and the resulting brain damages can be mitigated. [vii] This is highly significant, because – besides the cytokines – the spike protein of covid-19 can cross the blood-brain barrier and induce inflammatory processes in the brain leading to neuroinflammation and neurological disorders. [viii] [ix] [x] Elderly patients with chronic diseases have impaired vagus nerve activity that may exacerbate the covid-19 disease course. [xi] For this reason, methods increasing the vagal tone may be beneficial for the treatment or prevention of the severe consequences of covid-19 infection. One of the most promising methods is the intranasal administration of proinsulin c peptide. Systemic administration of C can increase the vagus nerve activity according to clinical trials on insulin-dependent diabetes mellitus patients that are among the most affected people regarding the mortality of covid-19 caused disease. [xii] [xiii] Proinsulin c peptide administered directly into the brain seems to have even a more pronounced effect on the parasympathetic nervous system. [xiv] Intranasal application of proinsulin c peptide is effectively transferring the peptide into the brain. [xv]
The resident immune cells in the CNS, the microglia, are often activated in patients severely affected by the disease according to autopsic investigations. [xvi] The hyperactivity of the molecular scissor, cofilin that regulates the shape and dynamical change of the actin cytoskeleton is responsible for the overactivation of microglia. The reduction of the hyperactivity of the cofilin is leading to the cessation of the overactivity of microglia. [xvii] [xviii] Interestingly, proinsulin c peptide, besides increasing HRV, is also able to inactivate cofilin in lymphocytes that may serve as a model for microglia and neurons also. [xix]
Description of the proinsulin C peptide spray
The participants of our study were using the Vargapeptide skin-spray off label, as an intranasal spray, on their own responsibility. The spray is produced and distributed by the Max-Immun Ltd.
This was applied in the same way as the intranasal insulin was and is administered in the population of children with Phelan-McDermid syndrome.
A 20 ml bottle contains a solution of 18 ml C-peptide. One puff off the spray contains 0,108 mg proinsulin C-peptid. In Vargapeptide 0,5 this amount is half of it, 0,05 g, in Vargapeptide 2 the amount is 0,216 mg.
The spray contains 0,8 % NaCl. The other ingredients fulfill the requirements of pharmaceutical grade purity. The purity of proinsulin C-peptid is 98-99%.
.
Description of the study
The effectiveness of C-peptide was investigated involving 30 patients with positive coronavirus test from the beginning of September to the end of December 2020.
- The investigated participants applied the C-peptide types 0.5, 1 and 2, each person the same type, mainly 1-1 puff every 4 hours, in case of severe symptoms 1-1 puff every 2 hours.
- the age of the patients ranged from 17 to 76 years
- the distribution of sexes was slightly more females (20) than males (10).
The investigated symptoms were divided into 3 categories:
Frequent symptoms: occurred in more than 9 cases
Moderately frequent symptoms: prevalence of 4-8 cases
Rare symptoms: reported in 1-3 cases
Other aspects of investigation:
- oxygen therapy
- mechanical ventilation
- anesthesia
Each patient started using the C-peptide spray within 3 days after being diagnosed.
The number, sex, age and comorbidity of the investigated paricipants
| Number of cases | Sex | Age (years) | Comorbidity |
| 1. | male | 17 | Hepatitis caused by Epstein-Barr virus o |
| 2. | male | 49 | Not known |
| 3. | male | 74 | Conn syndrome, hypertonia, arrhythmia |
| 4. | male | 31 | Not known |
| 5. | male | 61 | Not known |
| 6. | male | 67 | Morbus Chron |
| 7. | male | 34 | Not known |
| 8. | male | 68 | Not known |
| 9. | male | 30 | Not known |
| 10. | male | 55 | Not known |
| 11. | female | 53 | Hypertonia, diabetes type II. |
| 12. | female | 38 | Hypertonia |
| 13. | female | 44 | Thyroid disease |
| 14. | female | 50 | not known |
| 15. | female | 46 | Hashimoto thyroiditis, Insulin resistance, Joint pain |
| 16. | female | 39 | Autoimmune hyperthyroidism |
| 17. | female | 44 | Not known |
| 18. | female | 47 | Not known |
| 19. | female | 45 | Not known |
| 20. | female | 52 | Not known |
| 21. | female | 42 | Psoriasis |
| 22. | female | 54 | Hypertonia |
| 23. | female | 27 | Deep vein thrombosis |
| 24. | female | 49 | Asthma |
| 25. | female | 72 | Heart disease |
| 26. | female | 42 | Intestinal permeability syndrome Histamine intolerance, Adrenal fatigue |
| 27. | female | 40 | Not known |
| Number of cases | Sex | Age (years) | Comorbidity |
| 28. | female | 58 | Not known |
| 29. | female | 55 | Hypertonia |
| 30. | female | 57 | Not known |
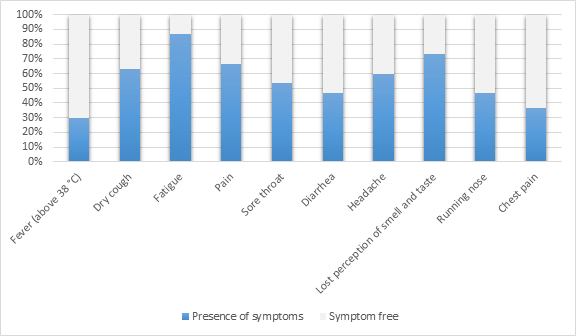
The group of patients with frequent symptoms
| Symptoms | Frequency | Percentage | Number of participants |
| Fever (above 38 °C) | 9 | 30% | 30 |
| Dry cough | 19 | 63% | 30 |
| Fatigue | 26 | 87% | 30 |
| Pain | 20 | 67% | 30 |
| Sore throat | 16 | 53% | 30 |
| Diarrhea | 14 | 47% | 30 |
| Headache | 18 | 60% | 30 |
| Lost perception of smell and taste | 22 | 73% | 30 |
| Running nose | 14 | 47% | 30 |
| Chest pain | 11 | 37% | 30 |
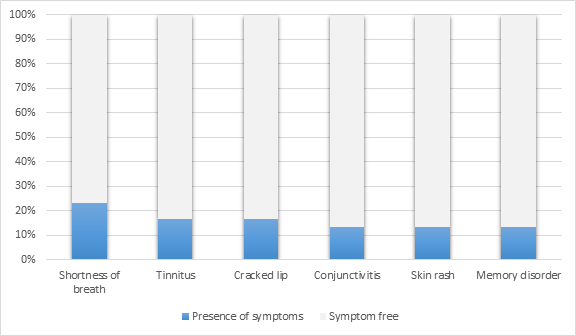
Group of patients with moderately frequent symptoms
| Symptoms | Frequency | Percentage | Number of participants |
| Shortness of breath | 7 | 23% | 30 |
| Tinnitus | 5 | 17% | 30 |
| Cracked lip | 5 | 17% | 30 |
| Conjunctivitis | 4 | 13% | 30 |
| Skin rash | 4 | 13% | 30 |
| Memory disorder | 4 | 13% | 30 |
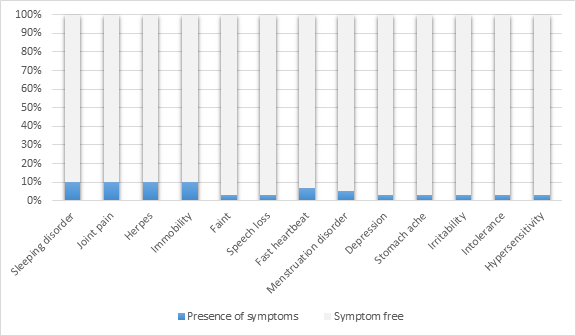
Group of patients with rare symptoms
| Symptoms | Frequency | Percentage | Number of participants |
| Sleeping disorder | 3 | 10% | 30 |
| Joint pain | 3 | 10% | 30 |
| Herpes | 3 | 10% | 30 |
| Immobility | 3 | 10% | 30 |
| Faint | 1 | 3% | 30 |
| Speech loss | 1 | 3% | 30 |
| Fast heartbeat | 2 | 7% | 30 |
| Menstruation disorder | 1 | 5% | 19 |
| Depression | 1 | 3% | 30 |
| Stomach ache | 1 | 3% | 30 |
| Irritability | 1 | 3% | 30 |
| Intolerance | 1 | 3% | 30 |
| Hypersensitivity | 1 | 3% | 30 |
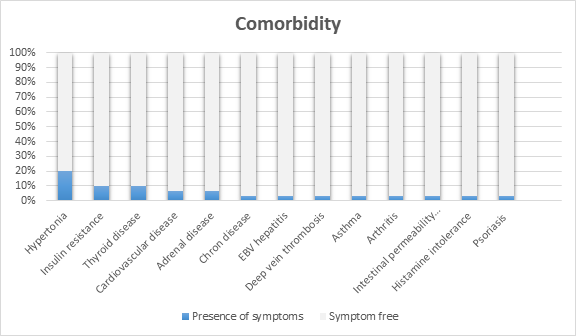
Investigation of comorbidity and returning to work
Returning to work
- Varied between 3-30 days, the average was cca15 days.
The proportion of persons with and without comorbidity was 1:1, among the 30 participants in the investigated group
There was comorbidity in 15 cases
| Symptoms | Frequency | Percentage | Number of participants | |
| Hypertonia | 6 | 20% | 30 | |
| Insulin resistance | 3 | 10% | 30 | |
| Thyroid disease | 3 | 10% | 30 | |
| Cardiovascular disease | 2 | 7% | 30 | |
| Adrenal disease | 2 | 7% | 30 | |
| Chron disease | 1 | 3% | 30 | |
| EBV hepatitis | 1 | 3% | 30 | |
| Deep vein thrombosis | 1 | 3% | 30 | |
| Asthma | 1 | 3% | 30 | |
| Arthritis | 1 | 3% | 30 | |
| Intestinal permeability syndrome | 1 | 3% | 30 | |
| Histamine intolerance | 1 | 3% | 30 | |
| Psoriasis | 1 | 3% | 30 |
Most frequently used antibiotic and antiviral drugs, supplementary treatments
In the group of investigated patients:
- hospital treatment became necessary in 1 case, this person was in deep anesthesia for 4 days (severe chronic disease: Conn syndrome)
- pneumonia int he early phase in 2 cases
- temporary vision loss in 1 case
- fluctuating blood pressure in 1 case
- overturning of the menstrual cycle in 1 case was observed.
Most frequently used antibiotic and és antiviral therapy:
- Azithromycin therapy 6 patients
- Favipiravir: 1 patients
- Isoprinosine: 1 patients
Blood thinner therapy: 2 patients(Clexane, Marfarin)
Symptomatic treatment: Algopyrin, Advil, Coldrex, ACC
Most frequently used vitamin, minerals and medicinal fungi (supplementary treatments):
Vitamin D: 24 patients
Vitamin C: 24 patients
Zinc: 13 patients
Magnesium: 6 patients
Tawny rose extracts: 3 patients
Propolis, L-Lysin, Silver-colloid, Quercetin, A-K2 vitamin, E-vitamin, Canabidiol, Ganoderma medicinal fungi extracts, Varga medicinal fungi extracts
The verbal feed-back of the investigated patients expressed a concordant opinion , that the above described symptoms rapidly relieved after introducing the c-peptide treatment, therefore their well-being significantly improved, also their hope for recovery. None of those who were treated with C-peptide were observed to have the most severe complications.
Literature related to the present investigation
[i] Gorham J, Moreau A, Corazza F, Peluso L, Ponthieux F, Talamonti M, Izzi A, Nagant C, Ndieugnou Djangang N, Garufi A, Creteur J, Taccone FS. Interleukine-6 in critically ill COVID-19 patients: A retrospective analysis. PLoS One. 2020 Dec 31;15(12):e0244628. doi: 10.1371/journal.pone.0244628. PMID: 33382773; PMCID: PMC7774924.
[ii] Ahnach M, Zbiri S, Nejjari S, Ousti F, Elkettani C. C-reactive protein as an early predictor of COVID-19 severity. J Med Biochem. 2020 Oct 2;39(4):500-507. doi: 10.5937/jomb0-27554. PMID: 33312067; PMCID: PMC7710381.
[iii] Huston JM, Tracey KJ. The pulse of inflammation: heart rate variability, the cholinergic anti-inflammatory pathway and implications for therapy. J Intern Med. 2011 Jan;269(1):45-53. doi: 10.1111/j.1365-2796.2010.02321.x. PMID: 21158977; PMCID: PMC4527046.
[iv] Haarala A, Kähönen M, Eklund C, Jylhävä J, Koskinen T, Taittonen L, Huupponen R, Lehtimäki T, Viikari J, Raitakari OT, Hurme M. Heart rate variability is independently associated with C-reactive protein but not with Serum amyloid A. The Cardiovascular Risk in Young Finns Study. Eur J Clin Invest. 2011 Sep;41(9):951-7. doi: 10.1111/j.1365-2362.2011.02485.x. Epub 2011 Feb 17. PMID: 21323913.
[v] Sajadieh A, Nielsen OW, Rasmussen V, Hein HO, Hansen JF. C-reactive protein, heart rate variability and prognosis in community subjects with no apparent heart disease. J Intern Med. 2006 Oct;260(4):377-87. doi: 10.1111/j.1365-2796.2006.01701.x. PMID: 16961675.
[vi] Frasch MG, Szynkaruk M, Prout AP, Nygard K, Cao M, Veldhuizen R, Hammond R, Richardson BS. Decreased neuroinflammation correlates to higher vagus nerve activity fluctuations in near-term ovine fetuses: a case for the afferent cholinergic anti-inflammatory pathway? J Neuroinflammation. 2016 May 10;13(1):103. doi: 10.1186/s12974-016-0567-x. PMID: 27165310; PMCID: PMC4894374.
[vii] Rhea, E.M., Logsdon, A.F., Hansen, K.M. et al. The S1 protein of SARS-CoV-2 crosses the blood–brain barrier in mice. Nat Neurosci (2020). https://doi.org/10.1038/s41593-020-00771-8
[viii] Olymaikolun, A. et al.: SARS-CoV-2 spike glycoprotein S1 induces neuroinflammation in BV-2 microglia, https://doi.org/10.1101/2020.12.29.424619
[ix] Achar, A.; Ghosh, C. COVID-19-Associated Neurological Disorders: The Potential Route of CNS Invasion and Blood-Brain Barrier Relevance. Cells 2020, 9, 2360.
[x] Prinsloo GE, Rauch HG, Derman WE. A brief review and clinical application of heart rate variability biofeedback in sports, exercise, and rehabilitation medicine. Phys Sportsmed. 2014 May;42(2):88-99. doi: 10.3810/psm.2014.05.2061. PMID: 24875976.
[xi] Johansson BL, Borg K, Fernqvist-Forbes E, Odergren T, Remahl S, Wahren J. C-peptide improves autonomic nerve function in IDDM patients. Diabetologia. 1996 Jun;39(6):687-95. doi: 10.1007/BF00418540. PMID: 8781764.
[xii] Barron E, Bakhai C, Kar P, Weaver A, Bradley D, Ismail H, Knighton P, Holman N, Khunti K, Sattar N, Wareham NJ, Young B, Valabhji J. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: a whole-population study. Lancet Diabetes Endocrinol. 2020 Oct;8(10):813-822. doi: 10.1016/S2213-8587(20)30272-2. Epub 2020 Aug 13. PMID: 32798472; PMCID: PMC7426088
[xiii] Okamoto S, Kimura K, Kitamura T, Cañas X, Yoshida T, Saito M. Proinsulin C peptide obviates sympathetically mediated suppression of splenic lymphocyte activity in rats. Diabetologia. 2000 Dec;43(12):1512-7. doi: 10.1007/s001250051562. PMID: 11151760.
[xiv] Derkach KV, Perminova AA, Buzanakov DM, Shpakov AO. Intranasal Administration of Proinsulin C-Peptide Enhances the Stimulating Effect of Insulin on Insulin System Activity in the Hypothalamus of Diabetic Rats. Bull Exp Biol Med. 2019 Jul;167(3):351-355. doi: 10.1007/s10517-019-04525-w. Epub 2019 Jul 26. PMID: 31346872.
[xv] Matschke J, Lütgehetmann M, Hagel C, Sperhake JP, Schröder AS, Edler C, Mushumba H, Fitzek A, Allweiss L, Dandri M, Dottermusch M, Heinemann A, Pfefferle S, Schwabenland M, Sumner Magruder D, Bonn S, Prinz M, Gerloff C, Püschel K, Krasemann S, Aepfelbacher M, Glatzel M. Neuropathology of patients with COVID-19 in Germany: a post-mortem case series. Lancet Neurol. 2020 Nov;19(11):919-929. doi: 10.1016/S1474-4422(20)30308-2. Epub 2020 Oct 5. PMID: 33031735; PMCID: PMC7535629.
[xvi] Alhadidi Q, Shah ZA. Cofilin Mediates LPS-Induced Microglial Cell Activation and Associated Neurotoxicity Through Activation of NF-κB and JAK-STAT Pathway. Mol Neurobiol. 2018 Feb;55(2):1676-1691. doi: 10.1007/s12035-017-0432-7. Epub 2017 Feb 13. PMID: 28194647; PMCID: PMC5554748.
[xvii] Shaw AE, Bamburg JR. Peptide regulation of cofilin activity in the CNS: A novel therapeutic approach for treatment of multiple neurological disorders. Pharmacol Ther. 2017 Jul;175:17-27. doi: 10.1016/j.pharmthera.2017.02.031. Epub 2017 Feb 20. PMID: 28232023; PMCID: PMC5466456.
[xviii] Aleksic M, Walcher D, Giehl K, Bach H, Grüb M, Durst R, Hombach V, Marx N. Signalling processes involved in C-peptide-induced chemotaxis of CD4-positive lymphocytes. Cell Mol Life Sci. 2009 Jun;66(11-12):1974-84. doi: 10.1007/s00018-009-9057-y. PMID: 19373435.
{kind=link}